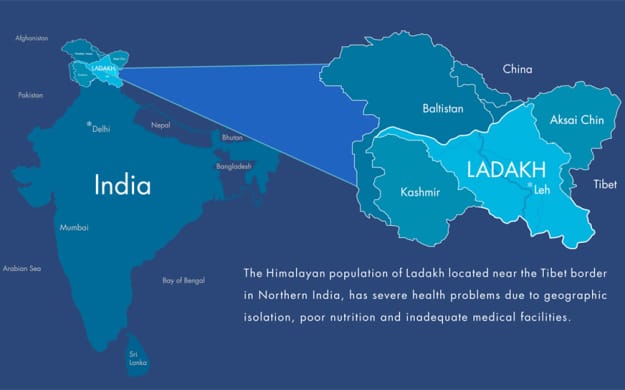
 Ladakh is a high altitude, mountainous land in the north of India and to the west of Tibet. Most of Ladakh is over 3,000 m above sea level. Due to its location in the middle of the Himalayas, much of Ladakh is a high altitude desert, as the Himalayas create a rain shadow denying the entry of monsoon clouds into the land. The inhospitable mountain environment means only 1,800 km of road have been laid in Ladakh - of which only 800 km have been surfaced. Currently, only two roads lead into and out of Leh, the capital of Ladakh, both of which are closed for the majority of the year due to snowfall at the high mountain passes. Other than the summer months, then, the only way to transport people or materials into or out of Leh is via air at the military airport in Leh. For other Ladakhis outside of Leh the situation is even worse. Many villages are not connected by road, and for those that are, many are submerged under snow for most of the year. For these villagers, should they need to reach Leh, they must walk many days through the mountain passes. In the winter this task is made considerably more difficult.
Due to its lack of arable land and its rugged terrain, Ladakh is one of the most sparsely populated regions of India. Historically Ladakh was comprised of the current districts of Leh and Kargil in Jammu & Kashmir, the Baltistan valleys and parts of the Indus valley to the west, the remote Zanskar region and Lahaul & Spiti to the south, Aksai Chin and Ngari to the east and the Nubra valley to the north. Contemporary Ladakh now lies entirely within the borders of Jammu & Kashmir, India’s northernmost state, with a geographical area of approximately 86,904 square kilometres. With a population of just 270,126, the population density of Ladakh is on par with countries such as Iceland and Mongolia – this in a country with a population of over 1.2 billion people. Ladakh has a strong Buddhist heritage and, indeed, historically, Ladakh has been more associated with Tibet than with India. For over a thousand years Ladakhi Buddhists would travel to Tibet for their Buddhist training in the great monasteries and throughout history Ladakh has been incorporated as a Tibetan vassal in various forms. Due to its geographic location close to the famous Silk Road, Ladakh, and the Leh region in particular, became important centres of trade - a role it still holds. To this day, for example, pashm, the material from which famous Kashmiri pashmina scarves and shawls are created, are predominantly imported from Ladakh. In the 18th and 19th centuries, after the Islamic and Sikh conquests of the region, Ladakh was introduced to the Indian sphere of influence where it has remained ever since. In more recent history Ladakh, due to its strategic location close to the Pakistani border, has been the site of several Indo-Pakistani wars. In 1949-1950 China invaded and occupied Tibet and simultaneously closed the Ladakhi-Tibetan borders - ending an important material and cultural trade route between the two lands. Since the Chinese occupation many Tibetans have fled to Ladakh which now hosts a sizeable number of Tibetan refugees. Since the Indian/Pakistani partition Ladakh has been a part of the Indian state of Jammu & Kashmir - a predominantly Muslim state administered from the state capital, Srinagar, in the far west of the state, in the Kashmir valley. Due to the differences between the needs of Ladakh and the other western districts of the state, many Ladakhis have requested the central government grant the land Union Territory status. Ladakhi's have a distinct religious, cultural and linguistic heritage. The Ladakhi culture with its strong Buddhist influence is an important component of the cultural mosaic that is modern-day India. In June 2016 the ATMA team, on request of the Ladakh Heart Foundation, conducted a 5 day research study throughout the Markha Valley in Ladakh. Traveling alongside a colleague from Delhi, himself a journalist in the field of development, I conducted extensive interviews and gained valuable quantitative and qualitative data on access to healthcare and health status. The Markha Valley has no roads, being cut-off from the rest of the district, and is only accessible by foot or mule. For many people in this valley, the closest medical facility is a 3 day hike away over treacherous rivers and high altitude passes. This inhospitable terrain places the inhabitants of the valley in greater danger in times of medical emergencies and the increased difficulty in accessing healthcare is believed to contribute to poorer health outcomes. This research trip provided the ATMA team and local NGOs with important data on the health status of residents within the valley and how this is related to the lack of access.
On a personal level this experience was a humbling one. Along the way we met people who suffered from many debilitating medical conditions who simply could not receive the care they deserved because facilities were not provided and the facilities that did exist were many days hike away. A formal analysis of the data is underway but from my firsthand experiences along this trek it was clear just how remote many parts of this district are and how this plays out in the day to day lives of inhabitants of the region. As always, once the data have been analyzed these will be shared on the ATMA website and with our NGO partners in Ladakh. In the meantime I have shared some pictures from the trip for the reader to envision in his/her mind the geographic constraints on healthcare accessibility in the region and to appreciate why we do the work we do in these areas of the world. Signing off for now. Indy ATMA President Introduction
Global health experiences (GHEs), or international health volunteering, known by a variety of names, is defined as a period of time wherein an individual (usually from the developed world) volunteers his or her time to help improve healthcare delivery (usually in the developing world). GHEs are becoming increasingly popular with both more organizations providing overseas volunteering opportunities and greater numbers of people involved in these ventures. These experiences are especially popular for medical students in the form of international medical electives during their pre-clerkship or clerkship education. Although GHE programs are growing there is limited research into the ethical considerations of overseas health volunteering and even less on the impact these programs have on the local communities they are designed to serve. The purpose of this paper was to review the literature on impact of GHEs, including a discussion on cost-effectiveness, as well as to analyze some important ethical issues related to international healthcare volunteering. Impact of GHEs on the local community GHEs are growing in popularity even though the research measuring the usefulness of these ventures is still lacking. By some estimates there may be as many as 100,000 NGO-sponsored volunteers (including healthcare volunteers) around the world per year. One study estimates that in sub-Saharan Africa alone there may be as many as 5,000 healthcare professionals operating there a year.1 The same trend is true of medical students opting to travel overseas as part of their training. A survey administered by the Association of American Medical Colleges noted a 33% increase in medical students embarking on GHEs from 2,838 students in 2001 to 3,799 students in 2009.2 The majority of volunteers who embark on these GHEs are young, educated, affluent and white which in itself raises some important questions. For example, does the fact that the demographic providing care is vastly different from the demographic receiving it have an impact on outcomes? How do these differences in demographics influence perceptions of ‘superiority’ in an international health field still struggling to shake off ties with its colonialist history?3 Many unanswered questions remain. The reasons for embarking on GHEs vary considerably. Many healthcare professionals and trainees embark on GHEs with the intention to use their specialized skills to help people. Others are drawn to the sense of adventure.4 Although well-intentioned, the individual who travels overseas on a medical mission with the goal of making a big difference in the community is probably misguided and certainly setting him or herself up for disappointment. This is especially true of GHEs that are shorter in length (and consequently smaller in impact). Many studies5,6,7 have found that short-term medical ‘voluntourism’ missions have little long-term impact in the community and may, in some cases, be harmful. Some concerns include 1) the ability to provide safe and effective medical services in the setting of language and cultural barriers that impair communication, 2) lack of follow-up care for patients who receive treatment, 3) increased burden on the hosting facilities (for both personnel and time), 4) providing medical care in a setting where practitioners are not held accountable for the consequences of medical interventions made, 5) the impact of short-term missions on the larger medical systems in the countries they visit and, 6) providing medical services that the community does not identify as being important to them. These concerns will be discussed in greater detail. The interaction between short-term medical missions and the larger medical system is complex and worthy of continued research. Previous studies have identified that to be most effective short-term medical missions should work closely with the recipient community and institutions.7,8 Working outside of the larger medical system can lead to local physicians having to duplicate work done by junior members of a foreign medical team to ensure it is done correctly. Many country experts view international health volunteers paradoxically considering that in many developing countries there is a surplus of unemployed local physicians and nurses who could do the same job for less cost. These experts argue that creating conditions for employment and training of national staff would be far more beneficial.1 It has also been suggested that groups providing free medical care in developing countries undermine the livelihoods of medical providers who depend on payment from these patients. This can lead to a breakdown in the relationship between the medical teams. One may argue that it is unethical to charge people in developing countries for medical services. However, a counterargument could be made that the people who truly cannot afford these services live in areas so remote international health volunteers seldom visit them. Instead, these volunteers spend most of their time in urban settings where many patients may indeed be able to afford the service. Foreign medical teams very rarely conduct socioeconomic evaluations to determine who should pay for these services even though this is something healthcare providers in developing countries believe should be done.7Foreign aid workers sometimes wrongly assume that because they’re in a developing country, everyone is poor. It has been proposed that having an individual in a developing country pay a nominal fee for health services delivered may be a good way to more actively promote involvement in one’s own care. Another pitfall of many health volunteering programs is the disconnect between what the program delivers and what the community identifies as being important. A 2009 study by Green et al surveyed 72 healthcare providers from the United States and Guatemala with experience in providing or hosting foreign aid health work.7 The authors highlight the importance of providing services that are relevant and useful to the community and are delivered in conjunction with local actors instead of in a parallel system running independently from the larger healthcare framework. In fact, the importance of short-term medical volunteers coordinating their activities with groups that have a long-term presence in Guatemala was by far the most frequently recommended point made by participants in the study. Short-term volunteers not doing so, in the words of one Guatemalan healthcare provider, “might as well stay home.” So, is it all bad news for GHEs? Not quite. Studies have shown there is value in long-term global health programs where groups are invested in the countries they work in and provide continued care. There is also some value in short-term missions, especially when they are working in conjunction with the larger health system; although the bulk of this value is probably reserved for the volunteers themselves. Surveys have identified that health volunteers appear to elicit the greatest benefit from short-term volunteer work overseas. A systematic review by Thompson et al compiled eight studies, including a total of 522 medical students and 166 residents who had completed GHEs as part of their training.9 They found that the GHE was associated with a career choice in underserved or primary care settings and with a positive effect on the trainee’s clinical skills, certain attitudes and knowledge of tropical medicine. The evidence would suggest that, at least for medical trainees, perhaps the greatest value in a medical elective is in its function as an educational adjunct. Suchdev et al, recognizing the pitfalls in short-term GHEs, have devised a set of principles to guide short-term medical groups in their overseas work.8 These seven guiding principles include: 1) a clearly defined mission, 2) close collaboration with the recipient community and its institutions, 3) a focus on sustainability, 4) education for the short-term team and the community, 5) service by addressing true health needs, 6) teamwork among short-term volunteers and, 7) a rigorous program evaluation. By following these principles short-term teams can have greater success in accomplishing their goals during their GHEs. Ethical considerations Needless to say, there are many ethical considerations that need to be taken into account when discussing GHEs. Although a thorough discussion of all of these issues is beyond the scope of this paper, below I have presented some of the more pertinent ethical issues that have been raised. Practicing out-of-scope medicine “The poor of the Third World are not experimental fodder.”10 Practicing a level of medicine that one would not normally practice at home has been raised by many as a serious ethical consideration that requires urgent attention.7,10,11 For practicing physicians this normally manifests as experimenting with new surgical techniques or treatment protocols. Much of the literature on this topic is focused on healthcare students, notably medical students. Medical students, who are pitched into an often-frenetic healthcare environment in the developing world constrained by limited resources and enormous demand, may believe it is justifiable to take on the role of a qualified physician.11 Much as a medical student pretending to be a qualified physician would be unethical and illegal at home, the same is true when students travel overseas. Medical students must be comfortable refusing to perform a task for which they have no training and to recognize their own limitations. They are morally obligated to do so. Banatvala et al suggest that medical schools should take the lead in developing clear guidelines for the scope of practice for medical students overseas which medical students should be familiar with prior to their electives. This idea has also been proposed by others.12 For medical students in Canada, the Canadian Federation of Medical Students (CFMS)13 has developed a pre-departure training program to help facilitate this. No matter where you are in the world, it is unethical to practice a scope of medicine that you are unfamiliar or uncomfortable with. Continuity of care One of the major ethical issues raised by GHEs is the lack of continuity of care7,10,14; especially for shorter-term volunteering experiences, which form the majority of GHEs. A study of anaesthesia care provided by Operation Smile volunteers5 found that although the complication rates associated with facial-cleft surgery was similar to rates in developed countries, the brevity of missions could contribute to avoidable illness and death. Indeed, these volunteers have been accused by local surgeons of neglecting these complications and leaving them for surgeons in the home institution to deal with once they leave. Some countries now have regulations to encourage continuity of care for visiting foreign aid workers although limited resources mean these regulations are difficult to enforce.14 This ethical issue can be partially resolved by being involved in longer-term volunteer projects and mitigated completely by training the local healthcare staff. Training local staff would enable them to provide care that continues far beyond the mandate of any mission. Removing responsibility to improve health infrastructure In a study conducted by Green et al, healthcare workers in Guatemala identified dependency on foreign providers as a problem.7 The ethical dilemma raised here was that perhaps foreign teams who provide healthcare services remove or lessen the incentive for the national government to invest in healthcare for their own people. For example, the presence of multiple NGOs operating in a particular area may lead to the government believing the area is well served even if the quality is poor and service sporadic. Risks to overseas volunteers Several studies have examined the risks to volunteers traveling overseas.2,15,16 These studies note that volunteering overseas carries a substantial health risk and these risks need to be better understood and minimized. A study by Bhatta et al surveyed 219 individuals in the United Kingdom who had volunteered abroad with Voluntary Services Overseas (VSO).15 They found diarrheal diseases to be the most prevalent problem (79.9%) followed by skin and dental problems. Most of the volunteers stayed in regions with mosquito-borne diseases and 11.6% of volunteers had been diagnosed with malaria. Almost 25% of respondents reported experiencing aggression or violence during their mission. The authors of this study concluded that the health risks for volunteers are considerable and warrant pre-departure training and specific medical advice. Another study by Galvin et al examined injuries that afflicted medical students while on international medical rotations.2 They found that the risk of suffering from any sort of illness during international electives approached 50%; of which 19% sought care in their home country upon return. Most illnesses were self-limiting and relatively benign. The leading causes of fatality for these students were motor vehicle accidents and drowning. Particular attention should be drawn to the health risks associated with healthcare volunteers traveling overseas. Although research is limited in this field, one would expect that health risks are elevated in this group by virtue of their proximity to infectious agents in their work environment and often limited availability of personal protective equipment. Other risks could include HIV transmission due to needlestick injuries, infection from highly resistant microbial pathogens and aggression from patients. Risks associated with the hospital environment in the developing world require special consideration for this subgroup of volunteers. Cost-effectiveness of GHEs Data on the costs associated with GHEs are limited. Although the literature on impact of GHEs is growing, very few studies examine associated costs. Depending on the length of stay, the destination, whether the individual stays in an urban or rural setting and the complexity of the job at hand, the costs can vary considerably. Measuring the ‘effectiveness’ component of these experiences when trying to determine cost-effectiveness is much more abstract and far more difficult to quantify. In this section I will, therefore, discuss the costs alone. Most of the data available on costs associated with GHEs are from surgical missions. The variability in costs associated with these missions can be considerable. Take, for example, the data on surgical missions for relatively simple procedures such as cleft lip and cleft palate repair (simple surgical procedures constitute the majority of overseas surgical missions). On a tight-budget, smaller-scale surgical missions wherein a handful of surgeons, anaesthesiologists and nurses travel with equipment to a developing world country can be performed for approximately US$10,000 per trip. Larger organizations such as Operation Smile, a charity that specializes in performing cleft lip and cleft palate surgery in low and middle-income countries, can have bills that run upwards of US$1 million.14 In 2002, a foreign surgeon performing cleft lip operations in Cambodia estimated the cost per operation to be US$1,000.10 For a two-week period in which a foreign team is able to perform 95 surgeries, this would theoretically cost US$95,000. Contrast this with an actual case in 2002 where, under the aegis of Handicap International, a team of local surgeons from Laos traveled to Pakse in southern Laos to perform cleft lip and palate operations. The total, all-inclusive cost for 95 operations in a two-week period was US$7414, or US$78 per operation; a difference of US$87,568. The author of this editorial concluded that, “the money saved by not sending … people … could be used to establish funds to cover the cost of the operations performed by the local surgeons who have been trained by us. This way, with the same amount of money, if we remember the $80 U.S. versus the $1000 U.S. cost, it will not be 20,000 children with cleft lip and palate who would be operated on by visiting foreign surgeons but 240,000 children operated on by local surgeons who would have kept their dignity and would love us for it.”10 Literature examining costs for non-surgical overseas health volunteers is limited. One study by Laleman et al surveyed 13 international volunteer organizations that employed 2,072 full-time equivalent international health volunteers in 2005.1 Smaller organizations that sent volunteers for shorter times (2-3 weeks per mission) did not pay allowances and, therefore, reported significantly lower costs of approximately US$2,400; most of which went towards covering the costs of travel and housing. Larger organizations that paid allowances for longer-term missions reported costs of US$36,000 to US$50,000. Interestingly, the pay in most cases was not linked to experience or services-provided. For the 5,000 foreign health workers estimated to be working in sub-Saharan Africa during this period the total cost was estimated to be between US$180-250 million. Costs for medical students engaged in GHEs as part of their pre-clerkship or clerkship international electives also vary considerably depending on the destination and the organization they arrange with. Estimates for Canadian medical students are likely between CDN$3,000 and CDN$8,000 per one month mission. As physicians-in-training one could argue that medical students have even less impact on the local community which would decrease the cost-effectiveness of these GHEs (of course, this does not factor in the educational and other benefits to the student9). Conclusion GHEs are becoming increasingly popular even though the dynamic interplay between healthcare teams from the developed world and their counterparts in the developing world are not yet fully appreciated. As such there is a tremendous role for continued research in this area. This paper has highlighted some of the main components of GHEs including the impact they have on the local community, the ethical considerations that need to be addressed and their cost-effectiveness. In summary, GHEs are fraught with many issues that require careful deliberation. The healthcare provider or trainee that wishes to travel on a medical mission to the developing world should carefully and thoughtfully navigate these obstacles so that both they and the community they will serve stand to benefit. References
This review was written by Indy Sahota, President of A Thousand Metres Above (ATMA). It is for the reasons outlined in this paper that ATMA does not send volunteers overseas and has instead opted to pursue a more ethical and sustainable means of international development. Ladakh is an outlier, a black sheep, in a remote corner of the globe accessible only during a short summer season. It appeals to those on the fringe: Bikers ride thousands of kilometers on a roller coaster of a highway to reach this motorcycle Mecca, trekkers dare to scale its rugged mountains that almost touch the sky and writers like myself wander its steep curves in search of inspiration.
So much of what we hear about India is aspirational with global ambitions, but here I saw Indians concerned only with survival. Ladakhis looking to pass this summer and hoping the upcoming winter won’t be too harsh. People who were simple and content with little that life has to offer. Surprisingly, this India is happy, warm-hearted and welcoming. Indy, a young doctor, and I trekked to Ladakh’s remote villages and spoke to people cut off from the mainstream consciousness. We were lost and we were found on the mountains of Ladakh. Sunset near a stream in Skiu village After a day spent acclimatizing in Leh, we decided to explore Markha valley and learn about the healthcare conditions in the region. It was part of Indy’s missionary zeal and I was happy to play a supporting role. The beginning of the five day trek was as dramatic as any Mission Impossible movie. Indy and I hopped into a rickety wooden trolley (hanging twenty feet above a free flowing river) supported by a flimsy cable rope. We were two idealistic men way over our head. During the 15-kilometer walk, I was constantly comparing Markha valley trek to the Great Lakes trek in Kashmir that I had taken in 2015. I was in search of pine trees and turquoise lakes, but there were none to be found. I couldn’t have been more foolish. There was a brown in Ladakh for every shade of Kashmir’s green. Tall, rugged mountains and a river that cut through them with grace. Sometimes we make this mistake: compare jobs, people and relationships. There are no comparisons in life, just different shades. An old lady with a toothless smile at Markha valley I sat on the floor of a small kitchen with a concerned mother, a shy daughter suffering from a brain stem problem and an extremely worried set of grandparents eager to help. Add to that a translator and two strange men (Indy and myself) asking personal questions. “She is a 25-years-old woman, but often behaves like a 12-year-old girl,” said Dorjee the translator, referring to one of the taunts hurled by the patient’s cousin. It was too much pressure and embarrassment and the girl began to cry. Indy stood there strong, asked a million questions, looked deep into her eyes, checked her hand and leg movements and reassured the family. “Nothing has changed,” he said to calm the teary-eyed girl. “You have lived 25-years without any problems. There is no reason why you should have any difficulties for the next 50.” It was reassuring. The 80-year-old grandmother scrambled to her room, brought two fine white mufflers and wrapped them around our neck. What a priceless gift; its tied around my backpack. I carry it with pride. The old lady had less than three teeth and a lovely smile. There was such kindness and love in her wrinkled face that I wanted to kiss her and somehow tell her how adorable she was. By the time we bid farewell, they were all smiling. I felt there was nothing more meaningful I could do with my life than help such families. Travel, travel, travel people say. It changes you. May be a little travel should be about changing the lives of others, for the better. The pain and pleasure of trekking in Hanker valley We came across a remote monastery on our way to Hanker Valley and decided to see it up close. The monk was too tired to accompany us and gave the key instead. The route was steep and we were completely out of breath by the time we unlocked the gates but I learned something on the way. Ninety-nine percent of trekking is painful and pointless. An endless walk leading to sore limbs and not even a pot to take a dump. But that one percent, when you come across a breathtaking place, a lone monastery on top of a hill, is extraordinary. It’s much the same with friendship, love and life in general. May be the proportions vary a little, but most of it is monotonous. It’s important to love that one percent enough to go through the grind. That evening, Indy and I had a long discussion about our past mistakes, present plans and dreams for the future. I slept morose that night thinking about all that I had lost. The darkness from the sky seeped through the window and found a way into my heart. But When I woke up, the Sun was shining bright, high up in the sky. I felt a surge of optimism within me. Life is like that, isn’t it? There are often dark times, wait for the sun and start walking. We were having lunch next to a lake when I heard the sound of thunder. The birds chirped in alarm and flew away to safety. There was rousing thunder in the sky and ominous dark clouds gathered around us. The weather had changed within minutes. It was only a matter of time before a hail storm began. The mountains that were moments ago brown in color were now covered by a white sheet. We rushed to the nearest camp site. Smoke came out of my mouth like a chimney. The local caretaker offered me a hot, steaming bowl of Maggie. All of us – Israelis, Canadians, French, Indians – were huddled inside a warm kitchen. So much for our differences. I thought of Orhan Pamuk’s novel, Snow and wished to write a poem of my own. If there is any good place to write a poem, its inside a tent, looking at the snow outside. Unfortunately, no such poem came to my mind. I was too cold both outside and inside. The highest pass with the greatest life lesson We had saved the best and the hardest for the last day. The ascent to the Kongmaru la Pass (5,300 meters) was demanding on the body and even more on the mind. With every step, the pass seemed to move farther away from us. I was out of breath within minutes. Add a hail storm to the mix and it became a battle for survival. I didn’t allow myself to look at the summit, instead I focused on the next ten steps. Four hours later, we were at the summit and the view was nothing like I had ever seen before and there was snow. The snowstorm and the freezing cold didn’t prevent me from writing down another priceless lesson. That pass, this trek taught me all I wanted to learn about life. You set yourself an impossible goal (a high pass) and inch your way towards it, step by step, like an ant. It doesn’t matter what your speed is, there are times when each step brings with it excruciating pain. Hail and snow make the path slippery, even dangerous but you have got to push past the pain barrier. Halt for a few seconds, look behind, see how far you have come already and continue onwards. The view at the top will be etched in your memory; the pain will eventually be forgotten. The descent back to reality When the dust settles and you head home unshaven, unshowered and unkempt. What’s left? A quiet confidence that says you can conquer the world. My lasting memory, what I took home wasn’t a trophy or a picture. It was the genteel smile of that old lady which carried hope and love. God bless her. Travel really has little to do with the destination, if at all, it’s about discovering something unique, hidden about yourself that gets lost behind in the daily madness of life. Anmol Arora New Delhi, India wordsbyanmol.com |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
November 2023
Categories |
 RSS Feed
RSS Feed